„Wir leben heute mit Krankheiten und Behinderungen, an denen wir früher gestorben sind.“
Sir Cyrile Chantler (2002)
In den letzten Jahren habe ich mich immer gefragt, warum das so ist?!
Wir leben heute in sehr merkwürdigen Zeiten, in denen der technologische Fortschritt zu einem endlosen Informationsangebot geführt hat, was wiederum zu einer Verbesserung der Lebensqualität führen sollte. Wenn wir auf das vergangene Jahrhundert zurückblicken, war die vielleicht größte menschliche Errungenschaft der bemerkenswerte Anstieg der Lebenserwartung. In den Vereinigten Staaten beispielsweise stieg die Lebenserwartung bei der Geburt in über 110 Jahren zwischen 1900 und 2010 von 47,3 auf 78,7 Jahre. Erstens resultierte diese zunehmende Lebenserwartung aus dem Rückgang von Infektionskrankheiten und Todesfällen, die sich auf junge Menschen konzentrierten. Die Lebenserwartung stieg in den letzten Jahrzehnten des 20. Jahrhunderts weiter an, was größtenteils auf die sinkende Sterblichkeit durch Herzkrankheiten zurückzuführen ist (Crimmins, 2015).
Länger zu leben bedeutet nicht, dass wir besser leben. Wenn wir uns die Studie von Park et al. (2018) genauer ansehen, die Prognosen zu Lebensjahren mit Behinderungen und Todesfällen aufgrund verschiedener chronischer nichtübertragbarer Krankheiten (NCDs) untersucht, können wir erkennen, dass diese Prognosen für 2030 in beiden Kategorien einen Anstieg bedeuten. Tabelle 1 fasst die prognostizierte Zahl der Todesfälle und altersstandardisierten Sterberaten für 21 Ursachencluster im Jahr 2030 im Vergleich zu denen im Jahr 2015 zusammen.
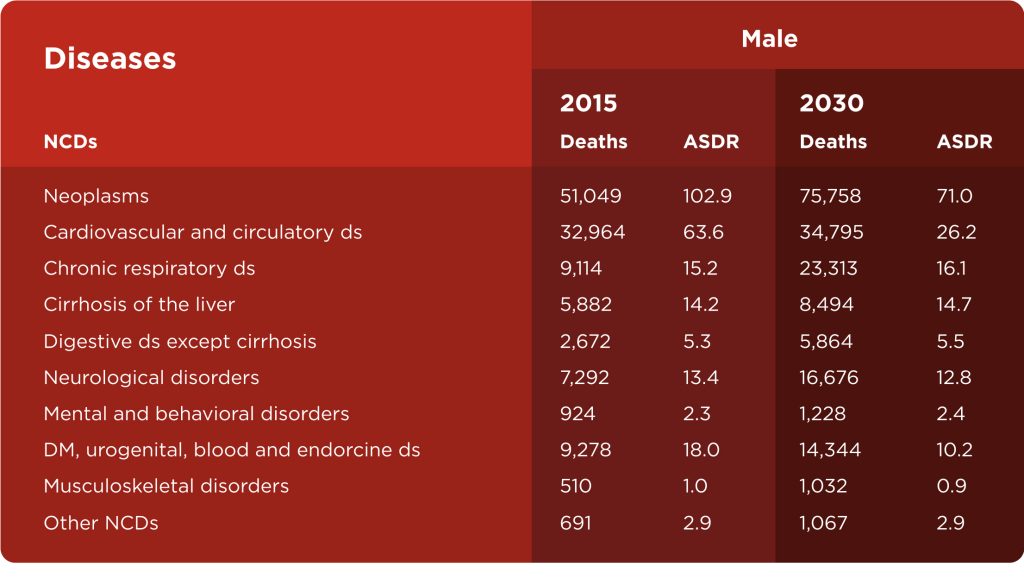
Chronische nichtübertragbare Krankheiten (NCDs) sind weltweit die häufigste Todesursache (60% aller Todesfälle) und sie sind für den jährlichen Tod von mehr Menschen verantwortlich als andere Ursachen zusammen. Die wichtigsten Arten von NCDs sind Herz-Kreislauf-Erkrankungen (wie Herzinfarkte und Schlaganfälle), Krebs, chronische Atemwegserkrankungen (wie Asthma) und Diabetes. Körperliche Inaktivität wurde als viertgrößter Risikofaktor für die globale Sterblichkeit (6% der Todesfälle weltweit) identifiziert und übertrifft sogar Fettleibigkeit und Übergewicht als Risikofaktor (Barbosa Filho et al., 2014). Muskel-Skelett-Verletzungen und Schmerzen (insbesondere Schmerzen im unteren Rücken) sind in diesem Zusammenhang mit NCDs und körperlicher Inaktivität wichtig, da sie eine der Hauptursachen für jahrelanges Leben mit Behinderung sind (Wu et al., 2020).
Wenn ich dies über das Coronavirus schreiben würde, wäre dies ein Thema, über das mehr gesprochen wird und das wahrscheinlich ein größeres Publikum und mehr Anerkennung finden würde, aber ich schreibe nicht über das Coronavirus. Ich schreibe über die Pandemie der körperlichen Inaktivität, über die Gesundheitsexperten schon sehr lange sprechen, aber es scheint, als ob dies nicht viel Erfolg bringt, da viele dieses Problem übersehen.
Was machen wir jetzt?
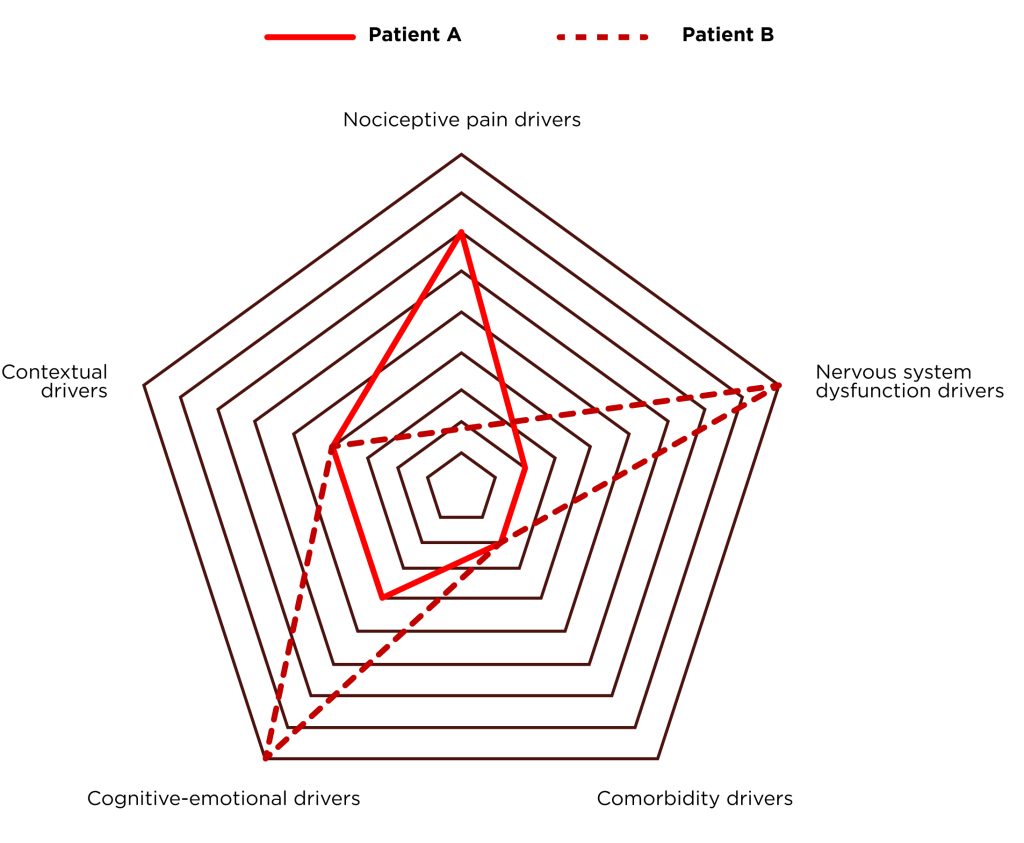
Als Team- und Einzeltrainer haben mein Team und ich im Laufe meiner Berufsjahre mit vielen verschiedenen Menschen mit unterschiedlichen Gesundheitsproblemen gearbeitet. Die meisten unserer Patienten leiden an Schmerzen des Bewegungsapparats, aber häufig leiden sie auch an anderen chronischen Krankheiten. Jedes Gesundheitsproblem und jeder schmerzhafte Zustand ist von Person zu Person unterschiedlich, und für jeden Patienten müssen wir einen anderen Ansatz verfolgen. Schmerz ist ein multifaktorielles subjektives Symptom, dessen Ursprung nur erklärt werden kann, wenn wir die Komplexität der verschiedenen Schmerztreiber und ihrer Zusammenhänge berücksichtigen (Abbildung 1). Die Welt der Fitness und Rehabilitation wurde in der Vergangenheit vom biomedizinischen Modell dominiert, und dieses Modell konzentriert sich auf die anatomische Pathologie. Aufgrund häufiger Fehler dieses Modells haben wir heute ein relativ neues Modell, das sogenannte biopsychosoziale Modell. Dieses Modell berücksichtigt zur Erklärung von Schmerz psychologische Faktoren (wie Angst und Überzeugungen), soziale Faktoren (wie Arbeitszufriedenheit) und nicht nur biologische Faktoren (wie pathoanatomische) (Liebenson, 2019).
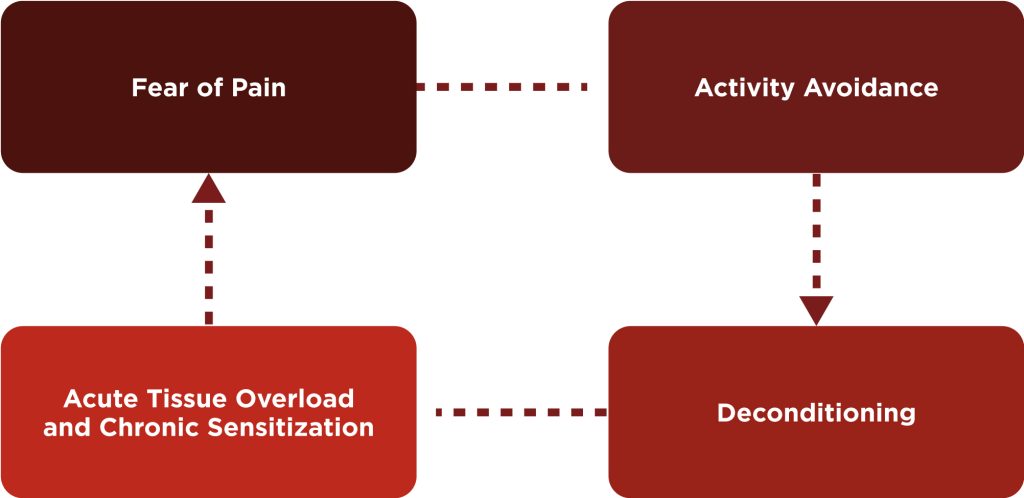
80% der Menschen leiden an einer schmerzhaften Erkrankung. Am häufigsten sind es Schmerzen im unteren Rücken. Es ist nicht schwer, bei diesen Personen ein gemeinsames Muster zu erkennen. Wenn eine Person Schmerzen hat, vermeidet sie häufig als Erstes Aktivitäten, was zu einer Dekonditionierung des Gewebes führt. Wenn eine Person versucht, zu normalen Aktivitäten zurückzukehren, erfährt sie eine akute Überlastung des Gewebes und häufig Schmerzen, was zu Angst vor Schmerzen und erneuter Aktivitätsvermeidung führt. Dieser Teufelskreis tritt häufig bei der Allgemeinbevölkerung auf, und die Mehrheit unserer Klienten war mindestens einmal Teil dieses Kreises. Die Aufgabe und das Ziel besteht darin, die Person mit Schmerzen aus diesem Kreis herauszuholen und ihr angemessene Unterstützung zu geben, um ihre schmerzfreien Ziele zu erreichen.
Unser Ansatz
Bewegung ist eine der wirksamsten Behandlungen zur Behandlung und Vorbeugung von schmerzhaften Zuständen und chronischen Krankheiten. Bewegungstherapie ist ebenso wirksam wie eine medizinische Behandlung und in manchen Fällen sogar wirksamer als eine medizinische Behandlung (Liebenson, 2019). Sie denken wahrscheinlich „Oh, da haben wir es schon wieder mit dieser langweiligen Sache mit Bewegung als Medizin“, aber als ich anfing, diesen Blog zu schreiben, stieß ich auf eine Studie von Pedersen und Saltin (2015). Die Daten aus dieser Studie waren überwältigend. Selbst ich hätte nicht erwartet, dass Bewegung einen positiven Einfluss auf so viele Gesundheitszustände haben würde. Kevin Carr von Mike Boyle Strength & Conditioning (einer meiner größten Einflüsse, um Fitness- und Kraft- und Konditionstrainer zu werden) sagte in einem seiner MBSC-Winterseminarvorträge, dass wir als Personal Trainer die „erste Linie der Gesundheitsfürsorge“ sind. Wenn wir einen Moment darüber nachdenken, fällt mir ein, dass, wenn eine Person hypothetisch alle zwei Monate zum Arzt geht (in meinem Alter ist das viel), der Arzt seinen Patienten 6 Mal pro Jahr sieht. Meine Patienten besuchen mich im Durchschnitt dreimal pro Woche, und wenn wir diese Informationen auf das Jahr hochrechnen, sehen meine Patienten mich 24-mal häufiger als ihren Arzt. Das ist einfache Mathematik. Wenn wir uns andererseits Metaanalysen genauer ansehen, die die besten Prädiktoren der Gesamtmortalität quantifizieren, können wir zu dem Schluss kommen, dass einer der besten Prädiktoren die kardiorespiratorische Fitness oder VO2max (Kodoma et al., 2009) und die Muskelkraft (Garcia – Hermoso et al., 2018) sind. Wir sind ein großer Teil des Gesundheitssystems, und diese Tatsache sollte stärker betont werden.
Wie ich bereits sagte, ist das biopsychosoziale Modell im Fitness- und Rehabilitationsbereich relativ neu und wir werden versuchen, es in die Praxis umzusetzen. Dies ist nur mit einem kundenorientierten Ansatz möglich. Dieser Ansatz befasst sich mit den Symptomen, Funktionsstörungen (Beeinträchtigungen, Fähigkeiten und Teilnahmemöglichkeiten) und psychosozialen Faktoren des Kunden (Beispiel 1).
Beispiel 1: Kunde X
- Symptom: Schmerzen im unteren Rücken
- Frühere Verletzungen: Schulterverletzung
- Funktionsstörungen:
a) Beeinträchtigungen: eingeschränkte Hüftstreckung, Hüft-IR, Schulterflexion, Plantarflexion und Schwäche der Hüftstreckung, hoher Ruhepuls
b) Funktionelle Fähigkeiten: Geh- und Sitztoleranz
c) Teilnahme: Arbeitstätigkeit - Psychosoziale Faktoren: Angst, Gegenstände vom Boden aufzuheben, Angst
Das größte Problem ist die heterogene Gruppe. Auf der einen Seite haben wir einen Kunden, der keinen Trainingshintergrund hat oder Schmerzen hat. Auf der anderen Seite haben wir eine fortgeschrittene Teilnehmergruppe mit hohem kardiorespiratorischem Fitnessniveau und Muskelkraft. In den letzten Jahren haben wir an einem Anpassungstrainingssystem gearbeitet, das Menschen zu den gewünschten Zielen führen kann. Ausgangspunkt dieses Systems und größter Einfluss waren Michael Boyle und sein Certified Functional Strength Coach. Sein Progressions-Regressionsmodell hat es ermöglicht, dass dieser Ansatz in Gruppenkonstellationen erfolgreich ist.
Basierend auf diesem Ansatz würde Klient X aus Beispiel 1 zunächst kein Kreuzheben mit externer Last machen, sondern Hüftbeugen für die richtige Kreuzhebetechnik. Als hüftdominante Kraftübung würde er Glute Bridges machen und dann zu einbeinigen Glute Bridges übergehen. Das berühmte Zitat aus Dan Johns Buch (2009) „Wenn es wichtig ist, tun Sie es jeden Tag“, also würde Klient X bei jeder einzelnen Trainingseinheit Schulter- und Hüftbeweglichkeitsübungen machen. Anhand seiner hohen Ruheherzfrequenzmessung und seiner Trainingshistorie können wir davon ausgehen, dass er eine geringe aerobe Kapazität hat, also würde er irgendeine Art von aerobem Training mit geringer Intensität machen, das seine Schmerzsymptome nicht verschlimmert. Heute wissen wir, dass Gehen und Ratschläge, wie man aktiv bleibt, genauso wirksam sind wie andere Behandlungen für unspezifische Schmerzen im unteren Rückenbereich (Artus, 2010). Der letzte, aber ebenso wichtige Punkt ist die Schmerzaufklärung des Patienten/Klienten, um Angst und Furcht vor Aktivitäten zu reduzieren.
Das Ziel
- Reduktion oder Beseitigung der Schmerzsymptome
- Reduzierung des Verletzungsrisikos beim Training oder bei alltäglichen Aktivitäten
- Progressive Verbesserung der körperlichen Fähigkeiten im Zusammenhang mit der menschlichen Gesundheit und Langlebigkeit (VO2max, Kraft, Flexibilität)
- Aufklärung der Klienten über Schmerzen und die Bedeutung von Bewegung zur Vorbeugung schmerzhafter Zustände und anderer chronischer Krankheiten
Botschaft zum Mitnehmen
- An die breite Bevölkerung:
Bleiben Sie einfach aktiv und treiben Sie wöchentlich Sport. Es muss Ihnen nicht gefallen, es muss sinnvoll sein. Ich laufe oder fahre nicht gern Fahrrad, aber ich mache es trotzdem, weil ich weiß, dass es mir auf lange Sicht gut tun würde. - An Fitness- und S&C-Trainer:
Betrachten Sie sich selbst nicht nur als Trainer, sondern als Heilpraktiker. Bieten Sie Ihren Klienten Bewegungsgesundheit und Sie können ihr Leben verändern. In meiner kurzen Karriere hatte ich das Privileg, mit mehr als 200 Menschen zu arbeiten, das sind 200 Gelegenheiten, jemandes Leben zu verändern. Vergeuden Sie das nicht!

Verweise
- Chantler C. „Der zweitgrößte Nutzen für die Menschheit“?. Clin Med (London). 2002
- Crimmins EM. Lebensspanne und Gesundheitsspanne: Vergangenheit, Gegenwart und Versprechen. Gerontologe. 2015
- Park B, Park B, Han H, et al. Prognose der verlorenen Lebensjahre, der mit Behinderung gelebten Jahre und der behinderungsbereinigten Lebensjahre in Korea für 2030. J Korean Med Sci. 2018;34(Suppl 1):e92. Veröffentlicht am 3. Dezember 2018.
- Barbosa Filho VC, de Campos W, Lopes Ada S. Epidemiologie von körperlicher Inaktivität, sitzender Tätigkeit und ungesunden Essgewohnheiten bei brasilianischen Jugendlichen: eine systematische Übersicht. Cien Saude Colet. 2014
- Wu A, March L, Zheng X, et al. Globale Prävalenz von Schmerzen im unteren Rückenbereich und Jahre mit Behinderung von 1990 bis 2017: Schätzungen aus der Global Burden of Disease Study 2017.Ann Transl Med. 2020
- Liebenson C.Rehabilitation der Wirbelsäule: Ein patientenzentrierter Ansatz. Dritte Ausgabe. Philadelphia: Wolters Kluwer; 2020.
- Pedersen BK, Saltin B. Bewegung als Medizin – Belege für die Verschreibung von Bewegung als Therapie bei 26 verschiedenen chronischen Erkrankungen.Scand J Med Sci Sport. 2015
- Kodama S, Saito K, Tanaka S, et al. Kardiorespiratorische Fitness als quantitativer Prädiktor der Gesamtmortalität und kardiovaskulärer Ereignisse bei gesunden Männern und Frauen: eine Metaanalyse.JAMA. 2009
- García-Hermoso A, Cavero-Redondo I, Ramírez-Vélez R, et al. Muskelkraft als Prädiktor der Gesamtmortalität in einer scheinbar gesunden Bevölkerung: Eine systematische Überprüfung und Metaanalyse von Daten von ungefähr 2 Millionen Männern und Frauen.Arch Phys Med Rehabil. 2018
- John D. Niemals loslassen: Eine Philosophie des Hebens, Lebens und Lernens. On Target-Publikationen; 2017.
- Artus M, van der Windt DA, Jordan KP, Hay EM. Symptome von Schmerzen im unteren Rückenbereich zeigen nach einer breiten Palette von Behandlungen in der Primärversorgung ein ähnliches Besserungsmuster: eine systematische Überprüfung randomisierter klinischer Studien.Rheumatologie (Oxford). 2010